


How Many Different Stages of Cancer
Though every case of cancer is unique to each individual, there are certain recognizable features that all cancers share. These features are used by doctors to accurately identify and determine which treatments will be the most effective.
For most types of cancers, physicians use staging information to assess the extent of the cancer, whether it has spread, and if so, where and how far. They also use cancer staging data to develop a plan for treatment and predict an individual’s prognosis (outlook).
Staging also provides physicians with a common language to effectively communicate about a patient’s cancer and collaborate with the multidisciplinary team of specialists on the best courses of treatment. There are other reasons for cancer staging as well, including to help identify any clinical trials that may be appropriate for you, your type of cancer, and its stage.
Terms and Definitions
As you learn more about your cancer diagnosis, you’ll come across many terms that are new to you and that you may not be familiar with. The NCI Dictionary of Cancer Terms from the National Cancer Institute has nearly 8,000 cancer terms searchable by first letter.
These terms are used to define and identify various aspects of cancer, and are used among medical professionals to identify and discuss the diagnosis and the treatments of cancer.
Albeit there are many terms associated with cancer, if you have been diagnosed with cancer, you will likely hear the following terms throughout your diagnosis, staging, and treatment:
Tumor: An abnormal mass of tissues that develop either when cells divide more than they should, or when they do not die. Tumors are either benign (not cancerous,) or malignant (cancerous.)
Biopsy: The removal of cells or tissues from a tumor, which are examined by a pathologist. There are several types of biopsy procedures, including:
- Incisional: Only a sample of the tissue is removed
- Excisional: An entire lump is removed
- Needle: A sample of tissue or fluid is removed with a needle
Grade: Also referred to as tumor grade and histologic grade, grading describes how abnormal the cancer cells and tissue look in a tumor, based on their appearance under a microscope. It also describes how quickly the cancer cells are likely to grow and spread. For each type of cancer, grading systems vary for each type of cancer, and are used to help determine the prognosis and plan treatment.
Metastasis: This term describes the spread of cancer from one area of the body to another. Tumors that form by cells that have spread are referred to as a ‘metastasis,’ or a ‘metastatic tumor.’ These types of tumors feature cells that are similar to those in the primary tumor.
In Situ: The origination point, or when abnormal cells are found only in their origination point. In other words, the cells have not spread.
Invasive Cancer: Also called infiltrating cancer, invasive cancer has spread beyond the layer of tissue where it developed and is growing into the healthy, surrounding tissues.
Lymph Nodes: Glands that fight illness and other invaders, including bacteria. They are located throughout the body and when cancer cells are found in the lymph nodes adjacent to the primary tumor, the cancer is more likely to spread throughout the body.
Prognosis: The suspected outcome or course of cancer, or the chance of recovery or recurrence.
Hyperplasia: The excessive growth of cells.
Ductal Carcinoma In Situ (DCIS): Cancer cells that haven’t grown outside of the site of origin. Also known as pre-cancer.
Benign: Not cancerous
Malignant: Cancerous
Oncologist: A physician that treats cancer.
Carcinogen: Substance that causes cancer.
Carcinoma: Cancer that arises in the epithelial tissue, or the outer layer of the tissue, such as the skin, the glands, or the lining of the internal organs. The majority of cancers are carcinomas.
Chemotherapy: A common treatment for cancer, which uses certain chemicals that kill cancer cells.
Radiation Therapy: A common cancer treatment, which uses high-energy rays to kill cancer cells.
Acute: Your cancer came on quickly and it is developing at a rapid pace, and will not last for a long period of time.
Bone marrow: Soft tissue that is located in the center of the bones where the blood cells form.
Invasive cancer: The cancer has spread outside of the location where it began and can potentially spread into other parts of the body. Invasive cancer is also known as infiltrating cancer.
Localized cancer: Cancer that remains confined in the area where it began. It has not spread into other parts of the body.
Questions to Ask Your Oncologist About Cancer Staging
Like most things, it is helpful to get some basic questions answered from your doctor once you’ve received a cancer diagnosis. Open communication between you and your primary oncologist and team of specialists is important in order for you to make educated and informed decisions concerning your treatment.
These are some basic questions you will likely want to ask regarding the staging of your cancer. Consider writing these down, and others, to bring with you to your appointment.
Question 1: What is the stage of my cancer?
Question 2: What does my cancer stage mean?
Question 3: Has my cancer spread to my lymph nodes?
Question 4: Has my cancer spread beyond my lymph nodes? If so, where?
Question 5: How is my cancer stage used in deciding on my treatment plan?
Question 6: Are there any clinical trials for my type of cancer?
Question 7: Should I get a second opinion on my cancer diagnosis and stage?
Question 8: Is the stage of my cancer treatable?
Question 9: What is the goal of my cancer treatment?
Question 10: How much time do I have before making a treatment decision?
Question 11: What is my prognosis?
If you are having difficulty understanding an explanation or answer to any question, ask for further clarification.
Note: The questions you choose to ask your doctor should be based on your unique situation, and your questions may change over the course of your cancer evaluation and treatment.
What is Cancer Staging?
In order to determine the rate of growth, doctors use what is referred to as a staging process. The prognosis and treatment of cancer are largely dependent on the stage of the cancer. In addition to staging, medical health professionals also use a variety of other factors to determine the prognosis and treatment of cancer.
These factors include:
- Your general health.
- The results of biochemical tests on cancer cells.
- Your individual preferences for treatment.
In general terms, cancer staging is based on evaluation of the size of the primary tumor, whether or not it has spread, and if it has spread, how far and where to. An accurate diagnosis of the stage of cancer is critical for effective treatment. Doctors use a variety of techniques and testing to determine the stage, including:
- Physical exams
- Imaging
- Lab test
- Biopsies
- Body fluid analysis
- Surgery
Once the stage of cancer has been identified, doctors have a precise way to determine and discuss your prognosis and treatment options with you and with other medical professionals.
Staging is pertinent to virtually all forms of cancer, excluding many different forms of leukemia. Leukemia involves the bold, which means that it is not anatomically localized, like other types of cancer. As such, the concept of staging for this type of cancer does not, and cannot apply.
The stage of cancer is usually based on four specific factors:
- The location of the primary tumor.
- The size and extent of the tumor(s).
- The involvement of the lymph nodes.
- Whether or not the cancer has metastasized (if it has spread to other, distant parts of the body).
Often, cancer is staged two times. The initial staging process is conducted prior to treatment. This is referred to as the clinical stage. The second staging process is conducted after treatment has been administered, such as chemotherapy or surgery. This is called the pathologic stage, and it is more precise to the extent of the cancer. The clinical and pathological staging process is discussed further on in this Ultimate Guide to Cancer Staging.
Why is Cancer Staging Needed?
The information that staging and grading offers helps medical professionals understand:
- Learn whether or not you need to have more testing.
- Understand the severity of your cancer and your survival rate, or how it will impact your overall health. .
- Accurately determine the prognosis, or the anticipated outcome and pattern of your illness.
- Plan the best course of action for your treatment; for example, if only chemotherapy is needed, or if a combination of therapies, such as chemotherapy and radiation therapy, are needed.
- Identify any clinical trials that may be helpful treatment options.
Further, cancer staging and grading provides doctors with a universal language, which they can use to effectively communicate with one another about your cancer. Medical professionals use staging and grading to determine the best treatment plan for your cancer.
In addition, cancer staging information is used by researchers when they study cancer treatments. It enables researchers to ensure that study groups are similar when they test different types of cancer treatments, and measure the outcome of treatments.
How Cancer is Staged
Different types of tests and exams are used in the staging process. The type of tests and exams that are used is dependent on the location of the cancer, and how much cancer is suspected. For example, in laboratory testing, tissues are removed from the body and doctors assess the tissues to determine how much the cancer has grown within this tissue. Imaging testing may also be used.
The following exams and tests are often used to stage cancer:
- Biopsies: A piece of the abnormal tissue, or tumor, is removed from the body, and is then analyzed under a microscope. Biopsies can either be done surgically, through a needle, or through an endoscope.
- Imaging tests: These tests provide doctors with a look inside the body and can pinpoint the location of the cancer, the size of the tumor, and if the cancer has spread. Common imaging tests used in the staging process include X-rays, CT scans, and MRI scans.
- Laboratory tests: Blood, urine, and other fluids and tissues are removed from the body and assessed.
- Pathology reports: These tests provide important information, including the size of the tumor, the growth of the cancer into other tissues and organs, the type of cancer cells, and the grade of the tumor (how closely cancer cells resemble normal tissue cells.) Pathology reports typically confirm the diagnosis of cancer, and its stage.
- Surgical reports: Samples of tissue are surgically removed from the body and are assessed. These reports determine the size and the appearance of the tumor. They also provide valuable insights about the lymph nodes and the involvement of other organs.
- Learn more about biopsy testing for cancer.
- Learn more about imaging tests for cancer.
- Learn more about laboratory tests for cancer.
- Learn more about pathology reports on cancer.
- Learn more about reading pathology reports on cancer.
Other Factors that Affect Cancer Staging
The tumor, the involvement of the lymph nodes, and whether or not the cancer has metastasized are generally the three main factors that are used in the staging process; however, they aren’t the only factors that can determine the staging process. Other factors that may be taken into consideration include:
- The grade: The grade of cancer measures the abnormality of the cancer cells. Abnormalities can be seen when tissues and cells are analyzed under a microscope. The grade is important because cancers with cells that are more abnormal looking have a tendency to grow and spread faster than those that do not have a large incidence of abnormal cells.
- Cell type: Cancer can be made up of different types of cells. Since all types of cancer cells can impact the treatment and the outlook of the disease, it can be a vital factor in the staging process.
- Location of the tumor: In some cancers, the location of the tumor can impact the outlook and the course of treatment. For example, in the case of esophageal cancer, the stage is dependent on where the tumor is located in the esophagus; the upper, the middle, or the lower third of the esophagus.
- Tumor marker levels: In certain cancers, tumor markers, or the blood levels of certain substances, can impact the stage of the cancer. In prostate cancer, for instance, the level of the prostate-specific antigen (PSA) in the blood is an important consideration in the staging process.
Types of Cancer Staging
Cancer is usually staged two main staging processes: The clinical staging process and the pathologic staging process.
1) Clinical Staging
This is the initial staging process. It occurs before any treatment is administered. The clinical staging process is an estimate of the degree of the cancer, which is based on a series of exams and testing results, including:
- Physical exams
- Imaging tests, such as X-rays, CT scans, and MRIs
- Tumor biopsies
Depending on the type of cancer a person is afflicted with, other test results may be factored into the clinical staging process, including blood tests, urine tests, and other fluid tests.
The clinical staging process is vital in determining the best treatment plan. Additionally, the clinical stage is the baseline that is used when doctors make comparisons when examining how the cancer reacts to the proposed treatment methods.
2) Pathological Staging
If surgery is performed on an afflicted cancer patient, the pathological, or surgical, stage of cancer can be determined. This cancer staging process is dependent on the outcome of the exams used in the clinical stating process, in addition to what doctors learn about the cancer during surgery.
Oftentimes, surgery is performed to remove the cancer and lymph nodes that are adjacent to the cancer; however, sometimes, surgery may be conducted so that doctors can see how much cancer is in the body, and to remove samples of tissue.
The pathological staging process provides medical professionals with more detailed information about the cancer, and this information can be used to make more accurate treatment plans and to better determine the prognosis.
Within these two main staging processes are cancer staging systems. Roman Numeral Staging and TMN Staging are applicable to most types of cancer, or cancers that have solid tumors. However, not all cancers can be defined by these systems. For example, blood cancers, like leukemia, do not have solid tumors, and therefore require the use of other types of staging systems.
Roman Numeral Staging
Roman Numeral Staging is used to describe the progression of cancer, and it is used with most cancers. In this staging system, the Roman Numerals I, II, III, and IV are used to identify the spread of the cancer. The higher the number, the larger the tumor and/or the more the cancer has spread.
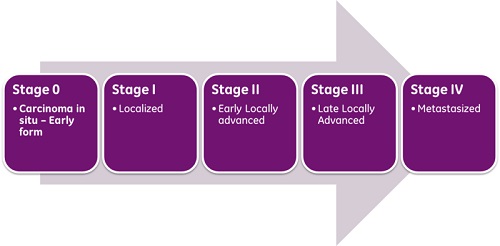
- Stage 0 – The earliest stage of cancer; it is present only in the layer of the cells in which the cancer began. Cancers in this stage are highly treatable.
- Stage I – The cancer is localized in one part of the body.
- Stage II – The cancer is locally advanced or has spread to and invaded other areas beyond the location where the cancer began.
- Stage III – The cancer is considered locally advanced, and is more advanced than Stage II.
- Stage IV – The cancer has spread to another organ.
Stages 0 and I cancers are considered to be the least advanced, and they typically have a better prognosis than cancers in more advanced stages. The higher the stage of the cancer, the more advanced it is; however, it is important to note that cancer in more advanced stages can still be treated, and can respond well to treatment. In other words, more advanced forms of cancer can successfully be treated.
TNM System: Cancer Stage
The TNM system is the most widely used staging classification system, and it is used by medical professionals around the world. This staging system is applicable to most solid tumor cancer types, such as colon, breast, and lung cancers.
This system was developed by, and is maintained by the AJCC and the Union for International Cancer Control (UICC.) The TNM staging system was created as a tool to help medical professionals better understand certain types of cancers, based on specific and standardized criteria.
In this system, cancer is classified in three stages:
T – Tumor
The size of the primary tumor is measured, and the extent to which it has spread to nearby tissues is determined.
| TX- | The initial tumor is unable to be evaluated. |
| T0- | No evidence of an initial tumor exists. |
| Tis- | The carcinoma (abnormal cells) in situ, or early cancer that has not spread to nearby tissues. |
| T1-T4- | The size of and the extent of the initial tumor. |
N – Lymph Node
Determines if, and how much, the cancer has spread to regional, or nearby, lymph nodes
| NX- | An evaluation of the regional lymph nodes cannot be done. |
| N0- | There is no evidence of regional lymph node involvement, or cancer has not been found in the lymph nodes. |
| N1-N3- | There is evidence that the regional lymph nodes are involved, or the number and/or extent to which the cancer has spread. |
M – Metastasis
Records whether the cancer has spread, or metastasized, to distant areas of the body.
| M0- | There is no evidence of distant metastasis, or the cancer has not spread to other parts of the body. |
| M1- | There is evidence that the cancer has metastasized, or the cancer has spread to other locations in the body. |
Oncologists assign each of these three categories with a number, which can range from 0 to 4 (T0 or N4). If evaluation of one of these elements isn’t possible, an X will follow the one of the letters. The three elements are then combined to identify the overall stage of the cancer, which is illustrated as 0 to IV.
Depending on the type of cancer, non-anatomic factors are also necessary to assign the anatomic stage or the prognostic group of the cancer. These factors are separately gathered from each stage of the TNM staging system, and they remain strictly anatomic. They are assigned to stage groups.
In the event that non-anatomic factors are used in groupings, a definition of the groupings will be provided for the specific case. For instance, if a non-anatomic factor is not available, an X will be assigned to that grouping.
In the TNM Staging System, a lowercase ‘c’ or ‘p’ is also used; ‘c’ denotes that the cancer is in the clinical stage, and ‘p’ denotes that the cancer is in the pathological stage.
Special Situations of the TNM Staging System
For brain tumors or central nervous system tumors, only the “T” section of the TNM system applies because the tumors usually do not spread outside the spinal cord or brain.
Oncologists stage most childhood cancers according to their specific types of cancer since the AJCC does not include pediatric cancers in its staging system.
Multiple myeloma, lymphoma, and leukemia cancers are not staged using the TNM system. Each of these blood cancers have their own unique staging system.
- Learn more about brain tumor staging.
- Learn more about multiple myeloma staging.
- Learn more about non-Hodgkin lymphoma staging.
- Learn more about Hodgkin lymphoma staging.
- Learn more about leukemia staging.
Other Cancer Staging Systems
While used more by registries, rather than physicians, another cancer staging system categories cancers into five main groups.
- In Situ – This meant that that abnormal cells are identified but have not spread to tissues nearby.
- Localized – Here cancer is limited to its origin, and has no spreading signs.
- Regional – This refers to cancer that has spread to nearby organs, tissues, and lymph nodes.
- Distant – Cancer has been noted to have spread to distant parts of the body.
- Unknown – The stage is undetermined because of lack of information.
Finding the Cancer Staging/Tumor Grading/ Changes in Cancer Stage
If you have been diagnosed with cancer, you likely have a lot of questions about your diagnosis. To learn more about your specific type of cancer, the first thing you need to do is collect information, including the following:
- The stage of your cancer.
- The grade of your cancer..
- The outlook of your cancer
This information will help you learn more about your prognosis.
Finding the Cancer Staging for Your Cancer
Cancer staging is a critical part of your prognosis. In order to find out and understand the staging system for your specific kind of cancer, the National Cancer Institute maintain PDQ Cancer Information Summaries for both Adults and Children categorized by the type of cancer in an alphabetical directory.
Tumor Grading
Tumor grading is another important factor that doctors use to determine the treatment options that are available for your specific type of cancer. Tumor grading measures the way abnormal cells from a tumor appear under a microscope, and the rate at which they seem to be dividing.
Generally, pathologists who assess cancerous cells classify them by assigning them a grade, which ranges from 1 through 4; however, specific types of cancers, such as breast and prostate, use a different type of grading system.
The lower the grade, the more similar cancerous cells are to healthy cells. Lower grade cancers are also less likely to grow and have a better chance of responding to treatment. Cancers that are assigned a higher grade have more abnormal cells, and there is a greater chance that the growth of the cancer will be more aggressive.
Changes in Cancer Stage / Restaging
When a diagnosis of cancer is given, the stage of disease is one of the first things that doctors determine. Once a stage is determined, it typically does not change.
In general, cancer is always referred to by the stage it was given when it was diagnosed. If the cancer grows or spreads, it will still be referred to by the original stage it was given. Any new information about how the cancer has changed will be added to the initial stage. While the cancer itself may change, the stage of the cancer usually does not.
Should the cancer grow, shrink, spread, or come back after successful treatment, its stage will remain the same as when it was initially diagnosed.
Your cancer is going to change, and these changes are documented, but they do not alter the stage of the cancer. Any new information about the cancer, including its size and whether or not it has spread, will be added to the initial stage.
In some cases however, medical health professionals may restage a cancer. Restaging helps doctors determine how well the cancer is responding to a specific treatment method. It also allows doctors to get more information about cancer that has come back after treatment. Restaging uses the same system that is used to determine the initial stage.
In restaging, if the new stage is determined, a lowercase ‘r’ will be placed before the new stage. This symbol illustrates that the new stage is different from the stage that was determined when the cancer was initially diagnosed; though it should be noted that this is not common.